COVID 19 Pandemic: Some Puzzles..
COVID-19 some puzzles
This article will be updated regularly...
Puzzle no.1 Lockdown and increasing numbers:
The main reason behind lockdown is to isolate the COVID positive people from other populations to avoid possible contact. For that, one should know who is affected and who is not. So testing comes first then tracing and then isolation of the COVID positive people and then Lockdown if required. What will happen if we don’t follow this order? If we lock down the state before testing and tracing, then it will increase the possible contact between COVID positive people and others as no one knows who is positive and who is not. Is that a reason behind the contaminated zone in India? Is that a reason behind the increase in the total number even after lockdown?
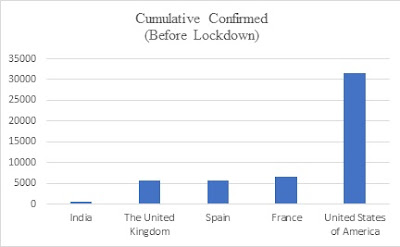
Data source: World Health Organization COVID-19 Global Data.
The number of confirmed cases is dependent on the number of testing done. As now every state is arguing that we have a high number of COVID-19 because testing is increased. So a high number of cumulative confirmed cases shows rapid testing while low number shows poor testing. India announced a national lockdown on 24th March where we have 519 cumulative confirmed cases. The main question: have we tested enough people (before lockdown), have we taken enough efforts to trace the people (before lockdown)?

Data source: World Health Organization COVID-19 Global Data (till 11th May 2020) (This number is not cumulative. These are per day cases)

Data source: Data is extracted from Our World In Data.
India before announcing the lockdown did very poorly on testing. Total testing per thousand is 0.015 and total tests are 20707 which is very low.
These four countries are witnessing the decline in new cases in the post lockdown period.

Data source: World Health Organization COVID-19 Global Data (till 11th May 2020)
While for India, it’s not declining.

It seems India has not reached the peak yet. The lack of testing and tracing in the initial period before locking down the economy may have created a situation where COVID positive person might not be traced but might be locked in the populated area.
Puzzle no. 2: Fatality Rate
There is a huge variation in the fatality rate as far as Indian states are concerned.

Data source: Ministry of Health and Family Welfare. Government of India, Extracted from Kaggle. the fatality rate is calculated based on the information available on 9th May 2020.
West Bengal has 9.5% the fatality rate while Kerala has 0.79% the fatality rate. But if we see the following table, then we can see that in West Bengal there are 1678 confirmed cases (cumulative).

Data source: Ministry of Health and Family Welfare. Government of India, Extracted from Kaggle. the fatality rate is calculated based on the information available on 9th May 2020.
As we discussed above, rapid testing means high cumulative numbers then West Bengal is not testing enough population. There is poor testing. How the fatality rate is calculated? the fatality rate=(number of deaths)/(total number of affected people)*100
Now if testing is low then the total number of affected people itself will be low and hence denominator will be low and hence the fatality rate will be high.

Data source: the fatality rate is calculated by using the data from the World Health Organization COVID-19 update (till 11th May 2020). The income categories are formed according to the classification done by the World Bank.
Till now, the average fatality rate is 4%. So now if I used that as a base then check the states above and below 4% then the mean total tests for India states above 4% (the fatality rate) is 62492.2 while for states with the fatality rate below 4% is 64775.57!!! They have tested less portion. Correlation is negative while states with a fatality rate below 4% are testing 1.3 people per 1000 while states with a fatality rate above 4% are testing 0.87 people per 1000.



Data source: Ministry of Health and Family Welfare. Government of India, Extracted from Kaggle. the fatality rate is calculated based on the information available on 9th May 2020.
So the question: Does West Bengal really have a high fatality rate or there is no enough testing?
Generally, the fatality rate is used to predict the possible casualty i.e. out of the total number of affected populations how much population can face the serious issue. But since we are not sure about denominator, let’s try to do the reverse process. Assume that the fatality rate is 4%. In West Bengal there are 160 unfortunate deaths So the total number of infected people might be 160*100/4=4000.
So in West Bengal, is testing very poor? Is it capturing only half the share of the infected population?
Puzzle no.3: Partial Lockdown
Does it make sense? Like in the contaminated zone, shops are opened for a few hours. This can invite the crowd. Let’s say there are 100 people and shops are opened for three hours. The probability of getting high people at the shop is very high compared to opening the shop for let’s say 8 hrs. So the question: Does partial lockdown make any sense? (Relax completely or don’t give any relaxation?)
Puzzle no.4: Vaccine vs existing health care
I will talk in detail about this puzzle in the next session. But assume that we have a limited pool of resources. Let’s say we have 100 Rs. And to fight the corona, we have two options. Put that money on Research and Development (like finding the vaccine or finding the medicine) with comes with uncertainty (we can’t predict the possible outcome) or Put that money on existing infrastructure like expanding the public hospitals, increasing the capacity, etc which has a calculated risk (we can predict the possible outcome). or make a balance between them. Here in the first option, the R&D is dominated by the private players while in the second option, we can talk about public institutional capacity. So question: By focusing more on the vaccine, are we incentivizing the private player to do R&D which comes with uncertainty? Can we focus more on the expansion of existing health facilities and infrastructure which has a risk regarding corona (calculated outcome) and has a certain outcome for the disease?
Puzzle no.5: Lockdown vs herd immunity
Can we separate the portion of the healthy population and can we artificially expose to the COVID-19 then isolate them? Let them recover. Again next portion.... The share of the population will be immune to the virus. The transmission depends on the total population (or population density). Since we are reducing the effective number of the population which will help to reduce the transmission. Yes, there are serious issues like how can identify who is healthy? Identification, Infection, Isolation, and Recovery all these are complicated processes. But this will help to reduce the efforts required for tracing and also possible transmission.
Can we separate the portion of the healthy population and can we artificially expose to the COVID-19 then isolate them? Let them recover. Again next portion.... The share of the population will be immune to the virus. The transmission depends on the total population (or population density). Since we are reducing the effective number of the population which will help to reduce the transmission. Yes, there are serious issues like how can identify who is healthy? Identification, Infection, Isolation, and Recovery all these are complicated processes. But this will help to reduce the efforts required for tracing and also possible transmission.

In the above picture, I tried to identify the number of people who are recovered and who aren't yet from the people who tested positive on the same day. The average days required for a person with mild disease is around two weeks (World Health Organization). So to get the approximate number of the composition, the number of people cured is subtracted from the total number of confirmed cases 9-10 days ago. This can approximately give the estimates about the composition of people who tested positive on the same day.
Now if a person is tested positive then the contacts of that person are traced, tested, isolated. Reports do take 2-3 days. Hence according to the proportion of the cured and non-cured population, the next two-three days new cases are divided into two-part. Those who come in contact with cured persons (i.e. cured in the next two weeks) and those who come in contact with a non-cured population. So if cured population (I assume that these cured people are healthy people) is isolated and exposed to the virus then the possible infection due to cured people can be avoided and once they recovered they are immune to the virus (Now it is unclear from existing studies that whether recovered person if he/she get infected again. can transmit the disease or not. Learning from other diseases, one can assume that the chances of transmission are very less from the recovered population) hence possible future transmission can be avoided.

If I try to compare the actual number of confirmed cases with a possible number of confirmed cases due to isolating the healthy people and exposing them, then we could have seen the flattened curve.
There are question marks over herd immunity. The herd immunity is achieved when the majority of population is infected by the virus so that the transmission will be stopped. Pollán et al. (2020) find that the majority of the Spanish Population is seronegative to COVID-19 infection. The study done on the larger sample suggests that around 5% population in Spain has witnessed the antibodies. Further, it is still not clear whether presence of antibodies protects the individual from getting COVID-19 infection again or not. But the question is why is a large population recovering from the COVID-19? More research will be done in these areas.
(One thing the people who are analyzing the pandemic should do: Rather than focusing on the modeling, mathematical, econometrical analysis, one should focus more on obtaining the large and effective data.
There are question marks over herd immunity. The herd immunity is achieved when the majority of population is infected by the virus so that the transmission will be stopped. Pollán et al. (2020) find that the majority of the Spanish Population is seronegative to COVID-19 infection. The study done on the larger sample suggests that around 5% population in Spain has witnessed the antibodies. Further, it is still not clear whether presence of antibodies protects the individual from getting COVID-19 infection again or not. But the question is why is a large population recovering from the COVID-19? More research will be done in these areas.
(One thing the people who are analyzing the pandemic should do: Rather than focusing on the modeling, mathematical, econometrical analysis, one should focus more on obtaining the large and effective data.
Reference:
Pollán, M., Pérez-Gómez, B., Pastor-Barriuso, R., Oteo, J., Hernán, M. A., Pérez-Olmeda, M., ... & Molina, M. (2020). Prevalence of SARS-CoV-2 in Spain (ENE-COVID): a nationwide, population-based seroepidemiological study. The Lancet.


.jpeg)
टिप्पण्या
टिप्पणी पोस्ट करा